
Understanding the diagnosis: Childhood visually impairing conditions
Presented on Thursday 1 November 2007
Ocular Conditions
Dr Andrew Blaikie, Consultant Ophthalmologist, Fife
Purpose of 'Lecture'
- Discuss the most common conditions that you see in your job
- Opportunity to ask questions and pick our brains
- Lots to talk about – can't cover everything
NOT the Purpose of 'Lecture'
- Tell you how to manage child from an educational point of view
- Suggest low vision management
- I'm not knowledgeable in that field
- Hopefully I can learn from you
References
- VIS or SSC website
- Dutton & Bowman book
- Taylor and Hoyt book
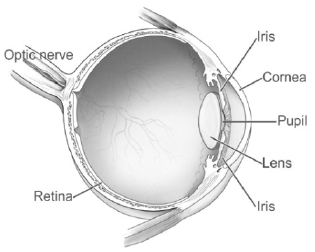
Anatomical Sites
- Whole Globe
- Cornea
- Lens
- Uvea (Iris, Ciliary Body and Choroid)
- Retina
- Optic Nerve
- Brain
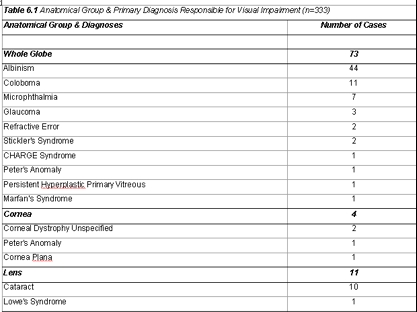
Whole Globe

Whole Globe
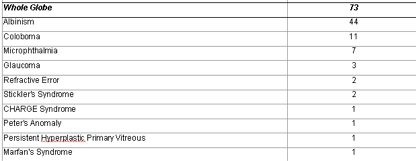
Albinism


Albinism
- Poor acuity
- Photophobia
- Nystagmus
- Dark glasses
- Hat
- Sunscreen
Genetics
- Chromosomes
- Autosomes
- Sex
- Inheritance patterns
Dominant
Recessive
X-linked
46 pairs of chromosomes
- 22 pairs of autosomes
(numbered by size)
- 1 pair of 'sex' chromosomes
(X or Y named by shape)
Dominant
- Only requires one copy of a misprinted gene for the condition to be expressed
- Males and females equally affected
- 1 in 2 children of affected parent will also be affected
- 1 in 2 will be normal and not carriers
- Don't really get carriers (but you can if disease is only weakly expressed)
Recessive Inheritance
- A 'recessive' condition to be 'manifest' requires both copies of the gene to be misprinted
- Affects male and females equally
- If only one copy misprinted then they are a 'carrier'
- If both parents carriers then 1 in 4 chance child will be affected
- 1 in 2 chance child will be carrier
- 1 in 4 chance neither affected or a carrier
X-Linked
- Males XY Females XX
- Most x-linked conditions 'recessive' so mainly boys affected
- Affected male will always pass on misprinted gene on X to daughters
- None of his sons will get his X and so none will be affected or carriers
Genetics
- Confused?
- Draw out the diagrams and stare at them and it makes sense
Nystagmus
- Congenital
- Acquired (usually adults)
- Sensory (eye problem)
- Motor Congenital (brain problem)
Nystagmus Symptoms
- Acquired: Oscillopsia and Reduced VA
- Congenital: only reduced VA
- Null point
- Abnormal Head Posture (AHP)
Nystagmus: Treatment
- Glasses
- Prisms
- Contact lenses
- AHP Surgery
Coloboma & Microphthalmia
Coloboma
- Part of eye missing
- Infero-nasal part
- Closure of embryological cleft
- Iris, retina, optic nerve


Microphthalmia

Issues
- How much vision
- Anything else wrong
- Retinal Detachment
- Orbit growth and facial symmetry
- Environmental cause?
- Genetic Counselling
Glaucoma
- Increasingly uncommon cause of childhood VI
- Early diagnosis
- Preventative treatment


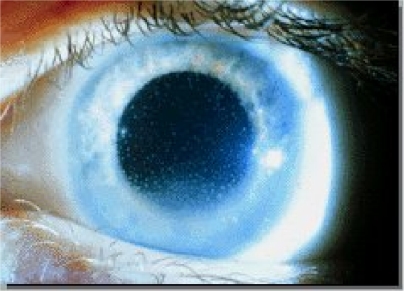
Cornea
Peter’s Anomaly

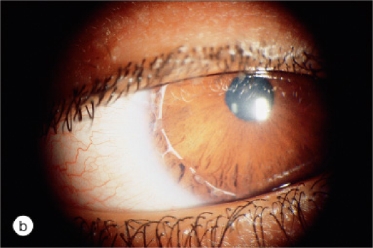
Lens
Cataract

Uvea
Aniridia

Uveitis
- 'Itis' means inflammation
- Uvea is coloured part of eye
Anterior : Iris
Intermediate: Ciliary Body
Posterior: Choroid

Retina

Retina
- Central Part of Retina: Macula
- Fine detail
- Colour
- Daylight

Photoreceptors: Rods
- No colour (because only one type)
- Poor acuity
- Work well in dark
- Movement
Photoreceptors: Cones
- Colour (because 3 different types)
- Fine detail
- Daylight
- Still
Macular Dystrophies

Stargardt’s Disease

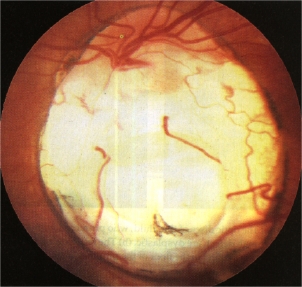
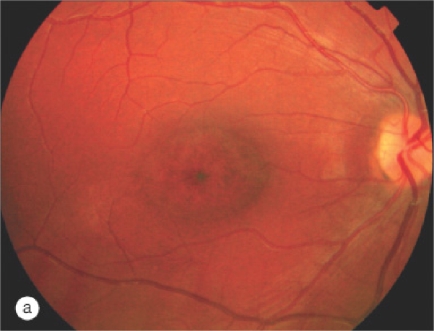
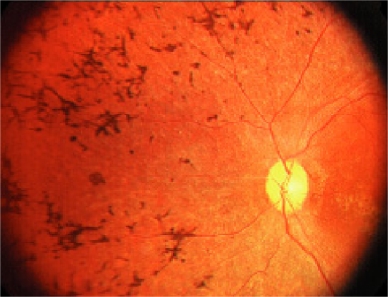
Retinitis Pigmentosa
- Description of appearance
- Disease of any part of the retina
- 'Progressive' rod and cone dystrophy
- Inherited
- Isolated ocular condition
- Associated with other conditions
- A syndrome
- Inherited condition
Symptoms
- Poor night vision: 'Night Blindness'
- Loss of peripheral visual field: 'Ring Scotoma'
- Gradual loss of visual acuity
- Catarcat
- Macular Oedema
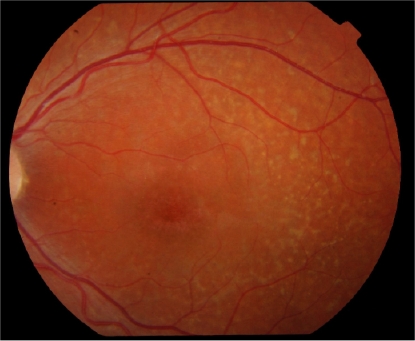
RP – mottled appearance

Leber's Congenital Amaurosis
- Non-Progressive Rod Cone Dystrophy
- Inherited
- Different types
- All photoreceptors badly broken
- Poor vision: often NPL
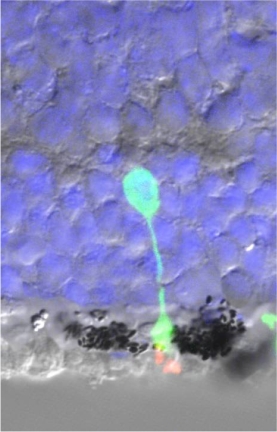
Any treatment?

transplanted cells

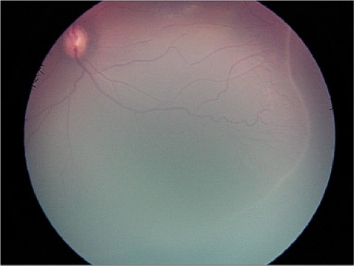
Retinopathy of Prematurity
- Blood system immature
- Parts of retina have no blood supply
- 'Ischaemic': leads to release of growth hormones (VEGF)
- Causes Damage: Retinal Detachment

Retinopathy of Prematurity
- Screening programme
<32 weeks
<1500 g - If ROP reaches a bad stage then treat
Treatment
- Laser or cold 'cryo' therapy
- Kills peripheral retina
- Switches off VEGF release
- Reduces risk of detachment by 90%

Survivors with no ROP may still have VI: Later problems
- Myopia
- Squint
- Amblyopia
- CVI (25% of premature babies have PVL)